When caffeine stops working, the problem isn't tolerance. It's that you've hit the ceiling of what your nervous system can sustain.
Most people experience this as a slow drift. The morning coffee that used to wake you up now just stops you from feeling worse. The energy drink that bridged the afternoon now leaves you crashed by evening. You add a second coffee. Then a third. The window of useful effect narrows. The crashes get worse. The baseline floor — what you feel like with no caffeine at all — keeps dropping.
This pattern isn't about caffeine becoming less effective. It's about what caffeine is doing to your autonomic system over time.
What caffeine actually does
Caffeine works primarily by blocking adenosine receptors in the brain. Adenosine accumulates throughout the day as a byproduct of cellular energy use. When it binds to its receptors, you feel tired. Caffeine occupies those receptors and prevents the tired signal from registering.
That mechanism is relatively benign on its own. The autonomic complication is downstream: when adenosine signaling is blocked, the sympathetic nervous system is released from one of its inhibitors. Sympathetic outflow rises. Heart rate climbs slightly. Cortisol releases. The body shifts into a higher-arousal state.
For an occasional user with a healthy nervous system, this is a useful tool. The system flexes into sympathetic activation, you get the cognitive benefit, the system returns to parasympathetic recovery, and the cycle repeats with full capacity each time.
For someone whose autonomic system is already running hot — chronic stress, poor sleep, persistent inflammation, structural drivers of sympathetic dominance — every caffeine dose is being added on top of an already-activated state. The system never gets to recovery. The ceiling drops over time.
The autonomic ceiling
Your nervous system has a finite capacity for sustained sympathetic activation. When the load exceeds the capacity, the system stops responding to additional input the way it used to.
This shows up clinically in a predictable pattern.
HRV drops, often into the 15-25 RMSSD range. Sleep becomes fragmented. Resting heart rate climbs. Anxiety levels rise even without an identifiable stressor. The "tired but wired" feeling — exhausted at the body level, unable to settle the mind — becomes a baseline state.
At that point, more caffeine doesn't produce more arousal. The receptors are already saturated. The autonomic system can't go any higher because it's already maxed. What you experience subjectively is that the coffee stopped working. What's actually happening is the system has lost its capacity to flex.
In short: Caffeine doesn't lose effectiveness through tolerance. It loses effectiveness when the autonomic system can no longer absorb additional sympathetic activation because it's already running at the ceiling. The ceiling is hardware, not willpower.
Caffeine and your nervous system
Stimulants are an input. In moderate, occasional use, they're an input the system handles without strain. In chronic, high-volume use on top of an already-loaded system, they become interference — they actively reduce the capacity of the nervous system to regulate itself.
The pattern looks like:
Input: Daily multi-source caffeine on top of poor sleep, chronic stress, and possibly structural drivers of sympathetic dominance.
Interference: Autonomic ceiling reached. The system can't downregulate to recover.
Output: Persistent fatigue, anxious floor, sleep disruption, crashes, dependence on more stimulants to get through the day.
The output looks like a caffeine problem. The driver is autonomic capacity, and caffeine is one of many things pushing against the ceiling.
What the warning signs actually are
The signal that you're approaching the autonomic ceiling isn't usually "caffeine isn't working." It's earlier than that.
Sleep that doesn't restore you despite sufficient duration. Waking at 3 or 4 AM with a racing mind. Resting heart rate creeping up over months. Tolerance for normal stressors dropping. Recovery from exercise feeling depleting rather than restorative. Anxious baseline that wasn't there a year ago.
When patients describe this pattern in the practice, the assessment usually confirms it: low HRV, sympathetic asymmetry on thermography, often a structural component contributing to chronic sympathetic activation.
The fix isn't quitting caffeine in isolation. The fix is addressing the underlying capacity problem — reducing the loads the system is carrying, restoring autonomic flexibility, fixing structural drivers when they're present.
Practical: how to read your own system
If caffeine has stopped working the way it used to, the productive question is: what else is loading my system?
Sleep quality and duration are usually first. Without recovery sleep, every other load compounds.
Chronic stress, including the unrecognized kind: sustained work pressure, caregiving load, ongoing health anxiety, accumulates over months and shows up as autonomic exhaustion.
Inflammation — dietary, infectious, environmental — adds load that doesn't feel like stress but functions like it from the autonomic system's perspective.
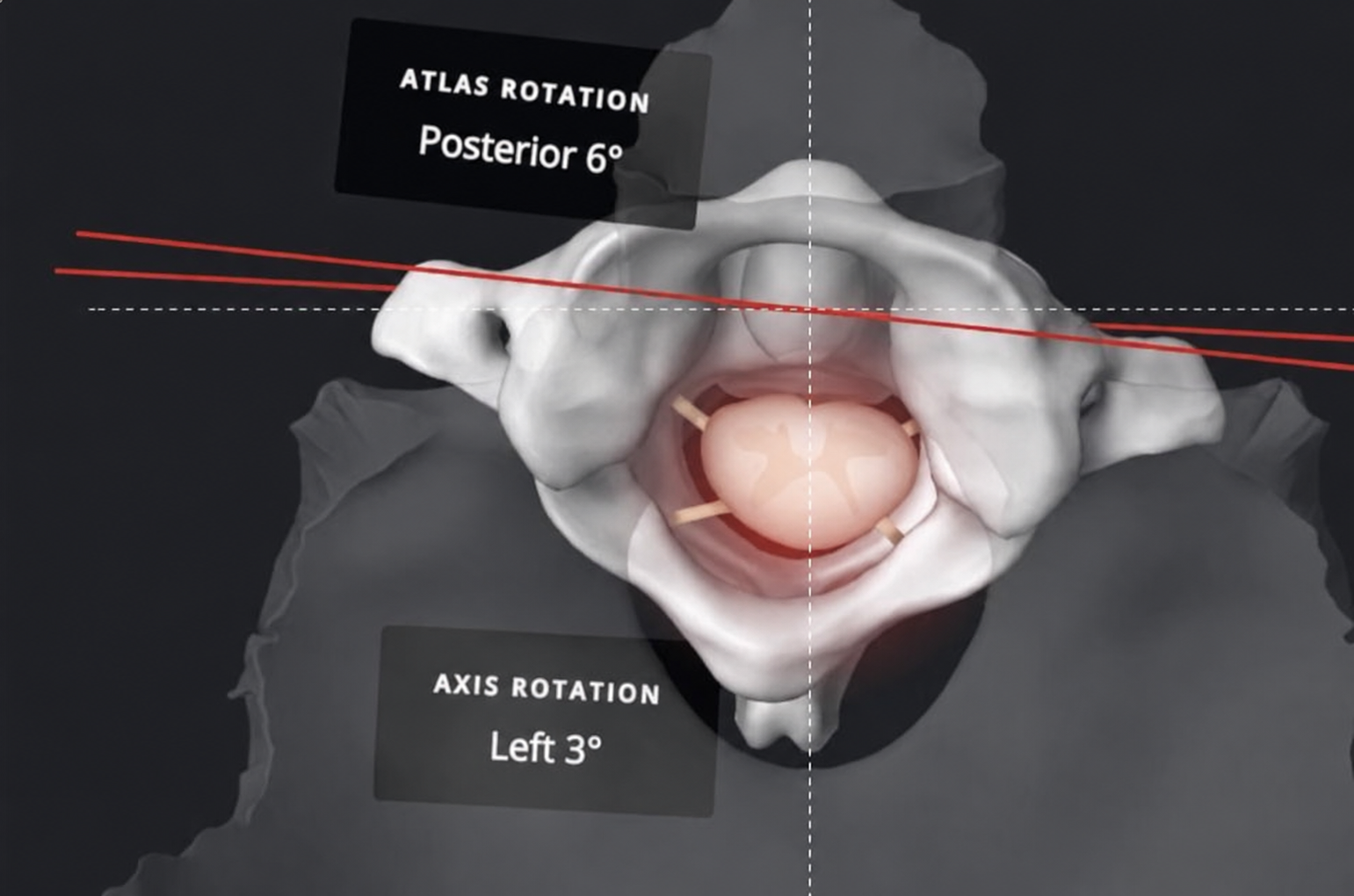
Structural drivers like chronic neck tension, post-concussion sequelae, and upper cervical misalignment keep sympathetic outflow elevated continuously. This is where structural assessment can identify a contributor that doesn't show up on any blood test.
Cutting caffeine acutely won't fix any of these. It just removes one input from a system that's overloaded elsewhere. Real recovery requires addressing the loads, not just removing the stimulant.
Schedule your assessment
If you've been running on caffeine for years and the system isn't responding the way it used to, the assessment looks at what's actually happening at the autonomic level. The first visit is a consultation, full assessment, and upper cervical x-rays. The HRV baseline alone often tells the story before anything else gets discussed.
Schedule Your Assessment Today.
References
1. Ribeiro JA, Sebastião AM. Caffeine and adenosine. *Journal of Alzheimer's Disease.* 2010;20 Suppl 1:S3-S15. doi:10.3233/JAD-2010-1379
2. Lovallo WR, Whitsett TL, al'Absi M, et al. Caffeine stimulation of cortisol secretion across the waking hours in relation to caffeine intake levels. *Psychosomatic Medicine.* 2005;67(5):734-739. doi:10.1097/01.psy.0000181270.20036.06
3. Shaffer F, Ginsberg JP. An Overview of Heart Rate Variability Metrics and Norms. *Frontiers in Public Health.* 2017;5:258. doi:10.3389/fpubh.2017.00258