Vertigo doesn't always start in the inner ear.
A meaningful fraction of the patients we see for persistent dizziness, lightheadedness, or "things shifting" sensations don't have a vestibular disorder in the classical sense. Their ENT workups come back clean. Their VNG is unremarkable. Their MRI shows no acoustic neuroma. And they're told it's stress, or anxiety, or "one of those things."
In a subset of these patients, the problem is the top of the neck.
What the upper cervical spine has to do with balance
Balance isn't one system. It's the integration of three streams of information: vestibular (inner ear), visual, and proprioceptive (joint and muscle position sense). The brainstem fuses these in real time so you know where your body is in space without thinking about it.
The upper cervical spine — specifically the joints where the skull meets the atlas (C1), and the atlas meets the axis (C2) — is the most proprioceptively dense region in the human spine. The deep suboccipital muscles contain a higher density of muscle spindles than almost anywhere else in the body. That density exists because the brain needs precise information about head position relative to the body to stabilize vision and maintain balance.
When that proprioceptive input becomes distorted, by altered joint mechanics, by chronic tension in the suboccipitals, by misalignment at the atlanto-occipital or atlanto-axial joints, the brainstem receives mismatched signals. Vestibular input says one thing. Proprioceptive input says another. The brain has to resolve the conflict in real time, and the resolution is often the sensation patients describe as vertigo, unsteadiness, or "brain fog with movement."
This is called cervicogenic dizziness, and it's been characterized in the clinical literature for decades. The neuroanatomy is established. The diagnostic challenge is that cervicogenic dizziness mimics vestibular disorders, and most workups don't include cervical proprioception assessment.
Why patients end up here after years of workups
The pattern is consistent. A patient develops persistent dizziness. They see their primary care physician. Referral to ENT. Hearing tests, VNG, sometimes ENG. Often a brain MRI to rule out structural causes. Sometimes a tilt-table test for orthostatic hypotension. The workups are negative or inconclusive.
By the time they come to a chiropractor, they've been told there's nothing wrong, or that it's anxiety, or that they should learn to live with it. They've often been on benzodiazepines or antihistamines for symptom management.
What's missing from that workup is an assessment of the upper cervical spine and its proprioceptive output. Not the soft-tissue tension assessment a manual therapist does, but a mechanical and neurophysiologic assessment of the joints between the skull, atlas, and axis. That assessment is not a standard part of vestibular workup, but for the cervicogenic dizziness subset, it's the key piece.
In short: Cervicogenic dizziness happens when the brain receives mismatched position signals from the upper cervical spine, and the brainstem can't reconcile them with vestibular and visual input. The result is dizziness with no inner ear pathology and no neurological lesion.
The mechanism: how atlas position affects balance
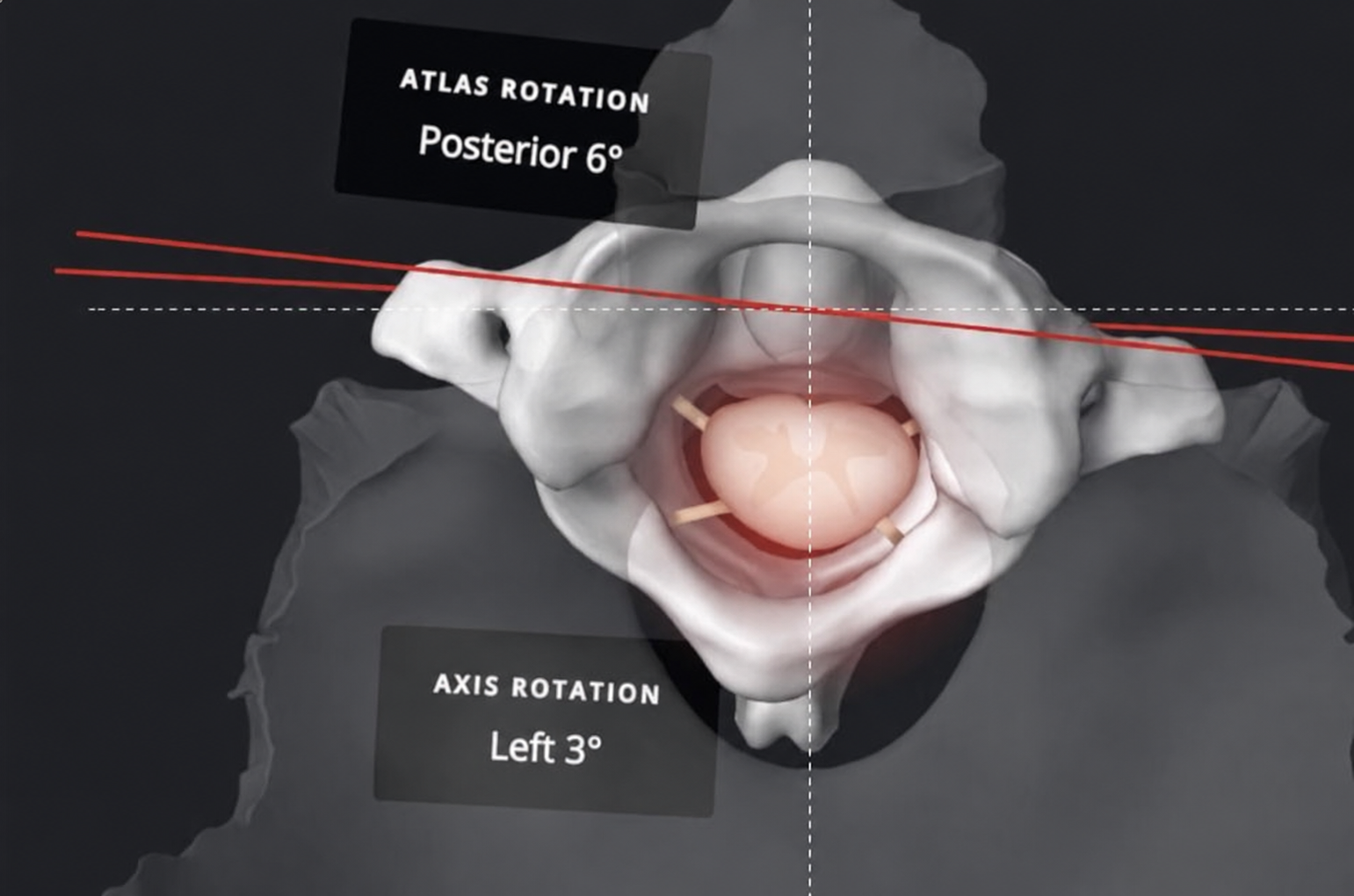
The atlas (C1) sits between the skull and the axis (C2). It carries the head and pivots on the dens of C2 to allow rotation. The joint surfaces are not load-bearing in the way the lumbar spine is. They're built for precision, not weight transfer.
When the atlas sits in a misaligned position relative to the skull and the dens, three things happen mechanically.
First, the joint capsules and the suboccipital muscles compensate to stabilize the head against gravity. That compensation creates chronic asymmetric tension. The brain receives constant abnormal proprioceptive input from those tissues.
Second, the vestibular nuclear complex, the brainstem region that integrates balance information, receives that distorted proprioceptive signal alongside normal vestibular and visual input. The mismatch is what generates the symptom.
Third, the autonomic nervous system, which has dense projections through the upper cervical region, becomes dysregulated. This is why patients with cervicogenic dizziness frequently also describe brain fog, nausea, fatigue, and difficulty concentrating. The vestibular complex doesn't exist in isolation. It's woven into autonomic regulation, and chronic vestibular-proprioceptive conflict drives sympathetic activation that patients experience as a generalized off-feeling.
Atlas Orthogonal restores the structural relationship between the skull, atlas, and axis using a precise, instrument-based correction. No rotation. No high-velocity manipulation. The correction is calculated from upright cervical imaging that measures the exact misalignment, then delivered with a percussive instrument that introduces a specific corrective force vector. When the structural relationship resolves, proprioceptive input normalizes, the brainstem signal mismatch resolves, and the dizziness resolves with it.
What the evidence shows
The strongest evidence for cervicogenic dizziness comes from the neuroanatomy itself. The density of proprioceptive afferents in the suboccipital region is established. The convergence of cervical, vestibular, and visual input at the vestibular nuclear complex is established. The capacity for cervical input to drive perceptual changes is established.
Clinical studies on manual cervical treatment for dizziness, including a systematic review by Reid and Rivett, show benefit for patients meeting cervicogenic dizziness criteria. Hain's clinical work has long differentiated cervicogenic dizziness as a distinct entity. The condition is in the differential diagnosis taught in vestibular medicine fellowships, even when it's underdiagnosed in primary care.
AO-specific outcome data on dizziness exists primarily as case series and clinical observation. The evidence base for the cervicogenic-to-vertigo mechanism rests on neuroanatomy, on convergent clinical observation across vestibular medicine and upper cervical chiropractic, and on the absence of competing explanations when standard workups are negative. Across the AO community, the clinical pattern is consistent: patients with persistent dizziness, normal vestibular workup, and identifiable upper cervical misalignment frequently improve with precise structural correction. That pattern is reproducible across practitioners.
What happens at Foresight when you come in with vertigo
The first visit is a consultation and full assessment.
The visit covers history, physical examination, and the full assessment workup. Thermography maps autonomic asymmetry in your skin temperature, which reflects the state of the sympathetic nervous system. Surface EMG measures muscle activation patterns in your spine, including the suboccipital region. Heart rate variability gives us a baseline of your autonomic flexibility, how well your nervous system shifts between sympathetic and parasympathetic states.
You also get upper cervical x-rays. Imaging is fundamental to the approach. The geometry of your alignment determines the corrective force vector for atlas orthogonal, and that geometry can only be measured from precise upright views. We don't estimate. We measure.
Between your first and second visits, the doctor reviews your imaging and assessment data. The corrective approach is calculated from the imaging measurements: angle, magnitude, direction of the misalignment. That calculation is what makes the technique precise rather than generalized.
The second visit is the report of findings. The doctor sits down with you, walks you through what the imaging and the assessment showed, explains what it means for your specific case, and outlines the treatment plan. When the assessment points to upper cervical involvement and the imaging confirms a misalignment, the first correction is delivered at this visit.
The correction itself is brief. You lie on your side. The Atlas Orthogonal percussion instrument is positioned based on the imaging-derived vector. You feel a brief tap. No rotation, no thrust, no audible cavitation. The force is calibrated and directional.
After the correction, we wait. We don't re-treat the next day. The nervous system needs time to integrate the new structural input. We typically reassess at 48 to 72 hours, then again at one week, then less frequently as the correction holds.
For cervicogenic dizziness specifically, the response timeline tends to be faster than for chronic pain conditions. Many patients report symptomatic improvement immediately. Some take a couple adjustments longer. A minority don't respond, which is the signal that the dizziness has a different driver and we should re-investigate.
Schedule your assessment
If you've been told everything looks normal but the dizziness hasn't resolved, the upper cervical assessment is the piece that's usually missing.
The first visit at Foresight is a consultation, full assessment, and imaging. We'll know within that visit and the doctor's review whether your case has a cervical component worth treating. If it does, the corrective plan is delivered at the second visit. If it doesn't, we'll tell you and point you where to go next.
Schedule Your Assessment Today.
References